Dengue
Key points
- The number of cases of dengue are increasing worldwide as are the number of countries with endemic infection.
- Dengue should be suspected in patients with a history of of recent arrival from or travel to an endemic country; sudden onset of high fever with signs/symptoms such as rash, nausea/vomiting, incapacitating myalgias or arthralgias, headache, leukopenia.
- There is no specific treatment for dengue; aggressive supportive care is required.
- There is a vaccine but it is not licensed in Canada nor is it recommended for travellers; prevention requires vector control and personal protection to decrease mosquito bites.
Epidemiology
Dengue is the most common viral disease transmitted by mosquitoes worldwide.1 It is caused by one of four Flavivirus serotypes (DEN-1, 2, 3 and 4), which are transmitted by Aedes mosquitoes, a day biting mosquito more often present in urban than in rural areas (Figure 1).1 These mosquitos bite especially in the early morning and in the evening before dusk. Before 1970, only nine countries had experienced severe dengue epidemics but this has changed with dengue now endemic in more than 100 tropical and subtropical countries around the globe especially in Asia, the Pacific, the Americas, Africa, and the Caribbean.
| Figure 1. Female Aedes aegypti mosquito |
 |
| Source: Centers for Disease Control and Prevention/Prof. Frank Hadley Collins, Dir., Cntr. for Global Health and Infectious Diseases, University of Notre Dame. Photo credit James Gathany. |
In 2013, the World Health Organization gave an estimate of about 400 million dengue infections per year with 100 million manifesting clinically and 22,000 deaths, mostly among children.3 The mortality rate for severe infection can be up to 15%, but is less than 1% with appropriate medical intervention.1 The rate of infection in young visitors or immigrants to Canada and in those returning from travel is not known, but anecdotal reports suggest an increase as the range of countries where Dengue is active increases. Dengue is now the second most common diagnosis in the returning traveller after malaria.2
Risk factors
Recent newcomers to Canada from a high-risk area may be at risk of infection, as are recent travellers to a high-risk area.
High-risk regions generally include tropical and subtropical regions, as shown in Figure 2.4
| Figure 2: Distribution of dengue risk, WHO 20164 |
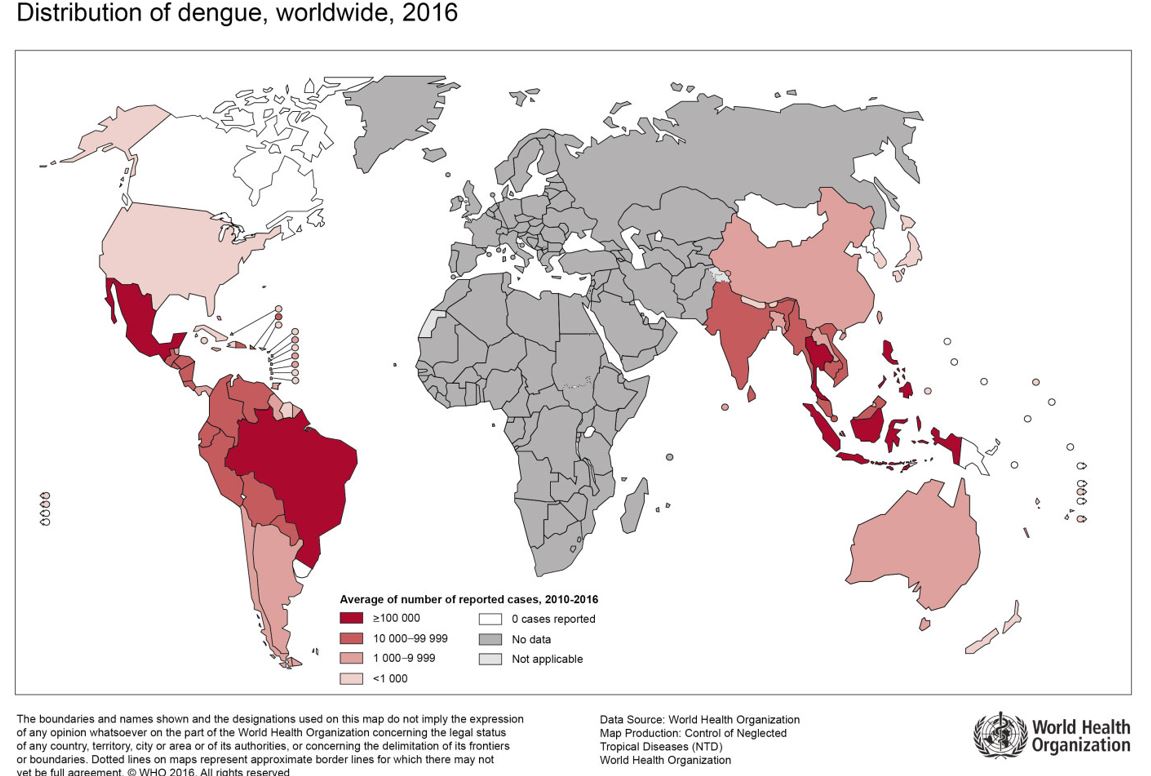 |
| Source: WHO Dengue Control – Epidemiology http://www.who.int/denguecontrol/epidemiology/en/ accessed Feb 22, 2018. |
| Risk Factors for Dengue Infection |
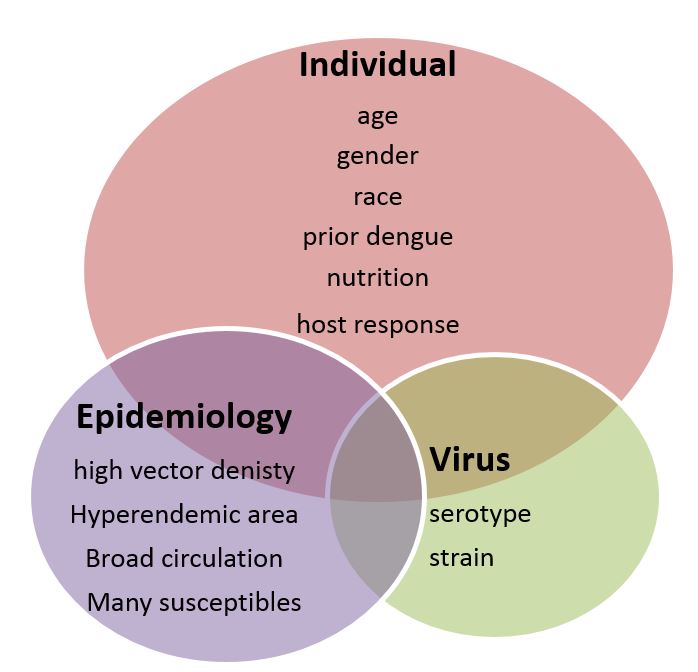 |
Clinical clues
Coming from or history of travel to an endemic country is key.
Signs of dengue fever generally develop 4 to 7 days post-infection but can occur as late as 14 days after the mosquito bite and may include:1
- "Break bone" fever
- High fever with sudden onset- often bi-phasic
- Severe headache
- Opthalmoplegia- retro-orbital pain
- Incapacitating myalgias and arthralgias
- Nausea
- Vomiting
- Rash appearing between fever spikes
- Occasional bleeding manifestations
- Leukopenia
Severity of infection
Recovery from infection by one Dengue serotype:
- provides lifelong immunity against that serotype,
- no protection to other 3 serotypes
Can be infected by up to four serotypes during their lifetime.
Small risk of severe disease after any dengue infection
- highest risk of severe dengue with second infection by a different serotype to the first
- Third and fourth infections usually associated with a milder clinical course7
- young age
- ethnicity
- possibly chronic diseases (bronchial asthma, sickle cell anaemia, diabetes)
Young children are at greater risk of dengue shock than adults because they may be less able to compensate for capillary leakage.4
Illness can range from non-apparent infection to classic dengue fever, severe dengue (previously known as dengue haemorrhagic fever), and dengue shock syndrome.1 Severe dengue is the leading cause of serious illness and death among children in some Asian and Latin American countries, outweighing malaria. The World Health Organization (WHO) has devised case definitions, but divisions between these definitions are often blurred.4
| Figure 3. Suggested dengue case classification and levels of severity4 |
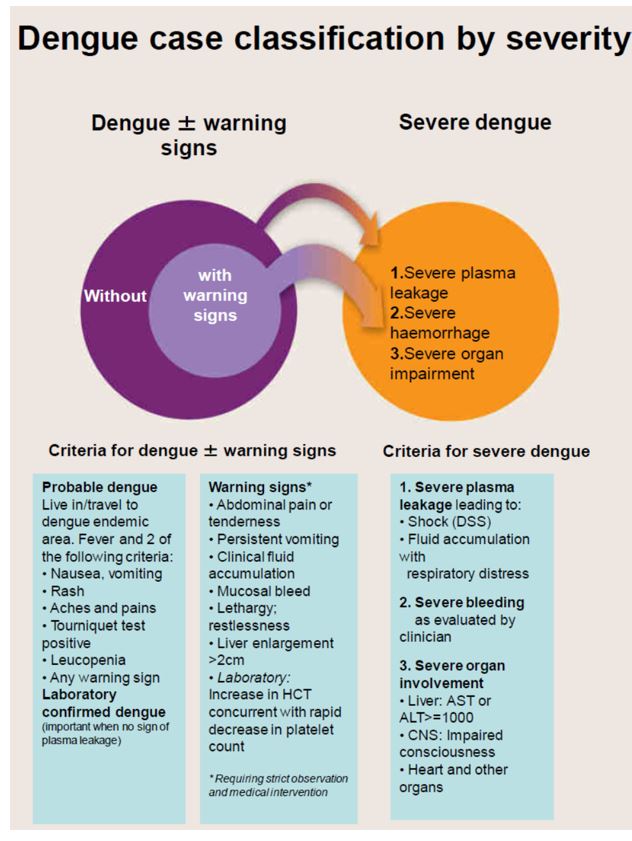 |
| Source: WHO. Dengue guidelines for diagnosis, treatment, prevention and control. Geneva, Switzerland: WHO, 2009: www.who.int/rpc/guidelines/9789241547871/en/ |
Diagnosis
Consider dengue in the differential diagnosis in patients with:1
- Fever
- And if coming from or history of travel to a risk area within 2 weeks of onset of symptoms
In such patients, need to consider malaria, dengue, typhoid fever, leptospirosis and influenza in the differential diagnosis.5
Criteria for diagnosis of dengue are noted in Figure 3.
Consider serological, molecular or other tests (e.g., antigen detection) to confirm diagnosis after talking to your laboratory, but recognize that there may be a delay in confirmation. Clinical decisions need to be based upon history and findings with confirmation coming later.
During the febrile period (especially in early stages), antibodies may not be present; during abatement of the fever, RNA, virion or dengue protein may be difficult to detect. The Committee to Advise on Tropical Medicine and Travel (CATMAT) recommends serological testing of acute-phase (collected 0 to 5 days from fever onset) and convalescent-phase (collected 6 to 30 days from fever onset) serum samples.1 The National Microbiology Laboratory in Winnipeg provides the diagnostic services for dengue in Canada.
Management
There is no specific therapy currently available for dengue.1 Management guidelines have been published by the WHO.4,6
Aggressive supportive care is required for serious disease.
- Due to capillary leakage, fluid management must be proactive and signs of shock recognized quickly.
- Bleeding must also be managed proactively and salicylates avoided, as they may exacerbate bleeding.
- Anticonvulsants may be required if seizures occur.
- Multi-organ failure may occur with liver, renal and cardiac involvement. Recovery may be slow and complicated.
- Long-term sequelae, such as cardiomyopathy and persistent fatigue, may occur.
Prevention
There is a vaccine against dengue (Dengvaxia ) but it is not approved in Canada nor is it recommended for travellers.7 Concerns have been raised about severity of disease with Dengue infection post immunization. Hence personal protective measures include reducing risk of mosquito bites through insect repellent and clothing cover for day biting mosquitos. Vector control is also helpful.8 Further information on prevention is discussed in the Travel-Related Illness section.
Selected resources
- Centers for Disease Control and Prevention. Dengue.
- World Health Organization. Dengue.
- Public Health Agency of Canada. Dengue. See also the Committee to Advise on Tropical Medicine and Travel (CATMAT). Statement on dengue. Can Commun Dis Rep 2009;35(April 2009):1-11.
- World Health Organization. WHO. Updated Questions and Answers related to the dengue vaccine Dengvaxia® and its use.
References
- Committee to Advise on Tropical Medicine and Travel (CATMAT). Statement on dengue. Can Commun Dis Rep 2009;35(April 2009):1-11.
- Chen LH, Wilson ME. Dengue and chikungunya infections in travelers. Curr Opin Infect Dis 2010;23(5):438-44.
- WHO. Dengue Control – Epidemiology. 2018. http://www.who.int/denguecontrol/epidemiology/en/ accessedFeb 22, 2018
- WHO. Dengue guidelines for diagnosis, treatment, prevention and control. Geneva, Switzerland: WHO, 2009: www.who.int/rpc/guidelines/9789241547871/en/
- Duber HC, Kelly SM. Febrile illness in a young traveler: Dengue fever and its complications. J Emerg Med 2013;45(4):526-9.
- WHO. Dengue and severe dengue. Fact sheet N°117. September 2013: www.who.int/mediacentre/factsheets/fs117/en/
- WHO. Updated Questions and Answers related to the dengue vaccine Dengvaxia® and its use. December 2017. www.who.int/immunization/diseases/dengue/q_and_a_dengue_vaccine_dengvaxia_use/en/
- Olliaro P, Fouque F, Kroeger A, Bowma L, Velayudhan R, Santelli AC, et al. (2018) Improved tools and strategies for the prevention and control of arboviral diseases: A research -to- policy forum. PLoS Negl Trop Dis 2018;12(2):e0005967.https://d oi.org/10.1371/journalpntd.0005967
Editor(s)
- Noni MacDonald, MD
Last updated: February, 2023