Immigrant adolescent health, Part 1: Background and context
Key points
- A significant proportion of young people in Canada are immigrants with particular health needs.
- Along with issues common to most Canadian adolescents, the processes of adaptation, social integration and identity development affect health in this group.
- Social determinants of health intersect with migration-related health influences.
- The influence of risk and protective factors also affect health outcomes.
- Risk factors include: Refugee status, trauma and exposure to violence, acculturation stress, differences in cultural beliefs between parents and children, single-parent families, discrimination and social marginalization.
- Protective factors include: Intact families, strong sense of identity within the family and at school, and an “integrated” acculturation strategy (i.e., the youth identifies with both their culture of origin and Canadian culture).
Introduction
Immigrant adolescents make up a substantial proportion of newcomers to Canada:
This page provides background and context on factors that affect immigrant adolescent health. For details on clinical priorities and recommendations for health professionals, see Immigrant adolescent health part 2: Guidance for clinicians
- In 2016, almost one in every 3 newcomers was under 24 years of age.1
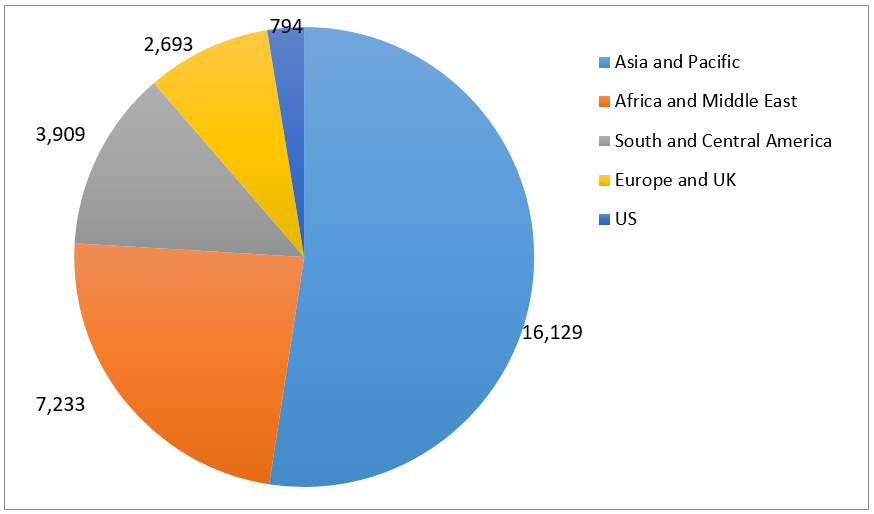
- About half of these youth are from Asia.2
- Most newcomer youth age 15 to 24 (79.8%) are from racialized “visible minority” backgrounds.3
Figure 1. Number of immigrants (permanent residents) new to Canada aged
15 to 24 years, based on region of origin, 20144
Immigrant adolescents face unique challenges that can have health implications. Adolescence is a critical developmental period, involving rapid brain development and specific physical, cognitive and social-emotional transitions and challenges that occur in different development stages.5 Important developmental tasks in adolescence include:
- Developing a sense of identity (individual and peer)
- Building relationships
- Acquiring the skills to cope with stress and life challenges.5,6
Adolescence is also a time to establish lifelong health behaviours that will profoundly affect physical and mental health into adulthood.5 Many immigrant adolescents may also experience specific challenges related to:
- The effects of their migration and resettlement experiences on identity development
- Stressors in their everyday lives, which can affect cognitive and physiological development
- Health risk behaviours
- Exposure to factors that shape health at a population level
Immigrant adolescents are a heterogeneous population with diverse and variable socioeconomic status, education and levels of social support. Population-based data should be interpreted with caution because research on broad groups such as “immigrant adolescents” or even “Asian immigrants” may obscure significant differences within groups, especially among small and marginalized subgroups: young people affected by trauma and political conflict (e.g., as refugees), poverty, violence, racism, discrimination and social exclusion.7
In clinical practice, health professionals should consider the length of time an adolescent has been in Canada and her immigration category (see category of immigrant) or refugee status. Both indicators influence degree of acculturation, migration and resettlement experiences, and may highlight a family’s reasons for immigrating.
Key terms
- Adolescent: A person age 10 to 19 years8
- Youth: A person aged 15 to 24 years9
- First generation: A person born outside of Canada who has migrated with or without their family to live in Canada
- 1.5 generation: A person born outside of Canada who arrives in middle childhood (6 to 12 years of age)10
- Second generation: A person born in Canada with at least one immigrant parent
- Newcomer: A person who has lived in Canada for less than 5 years
For definitions of immigration categories, see An Overview of Immigrants and Refugees in Canada.
A bullied adolescent from China
Ben has been referred to a local clinic. He came to Canada alone, about a year ago; Ben is living with a Canadian host family and attending high school while his parents continue to work and live in China.
At 15 years old, he is bullied at school and feels very alone. Ben is teased at school because of his accent when speaking English. He is struggling to feel “Canadian”, but no longer feels “Chinese”.
Ben is also bullied by other students who think he is gay. He is very upset and is questioning his own sexual orientation and identity. Recently, Ben told his parents that he might be gay, which they have found difficult to accept. They told him: “We don’t accept that in our family.” His father has not spoken to Ben for a month. Ben is anxious and scared about telling his host family about his emerging sexuality, because they have made derogatory comments about gay people. He feels isolated and emotionally distressed.
Questions to consider
What are a health care provider’s primary concerns?
- Social isolation
- Mood and anxiety symptoms, especially if related to discrimination and harassment
- Challenging experiences related to identity development: Sexual orientation, racial/ethnic identity, and acculturation
- Conflicts and poor connectedness with parents, likely related to cultural gaps
- Status as a “homestay” student (not living with parents) – a risk factor for decreased connectedness with parents
What are culturally competent next steps?
- Complete a HEEADSSS or SSHADESS assessment to evaluate Ben’s mental health symptoms, safety and suicide risk, including protective factors.
- Provide supportive counselling and/or connect Ben with appropriate mental health resources.
What services should Ben be connected with?
- School counsellor
- Culturally competent mental health services: Individual, +/- Family counselling (preferably with family members in China via telephone, with an interpreter)
- Immigrant youth or community groups
- LGBTQS2+ adolescent groups, organizations or services
- A clinician (preferably, in an adolescent medicine or adolescent mental health clinic) who will follow him serially and coordinate care
Learning points
The aim is to enhance Ben’s protective factors and reduce risk factors, at each level: individual, family and community. Assuring Ben that health care encounters are a safe and confidential place to explore experiences can help build the rapport needed for Ben to feel comfortable accepting support.
Individual interventions:
- Perform a developmentally appropriate, confidential adolescent psychosocial assessment (HEEADSSS or SSHADESS) routinely, but especially when there are psychosocial concerns
- Validate and support Ben around his stressors: Discrimination, harassment, family conflicts and identity development questions
- Perform a mental health assessment (including a safety assessment), and treat promptly or refer as needed
- Use affirming language to model inclusivity and comfort with Ben's sexual orientation
Family interventions:
- Have a confidential discussion with Ben about his evolving sexual identity: especially around disclosing to his biological and/or host families versus keeping his identity and experiences private
- If Ben wishes to disclose and discuss his sexual orientation issues with either or both families:
- Provide family-centred education and resources around adolescent mental health, identity development and sexual identity development.
- Advocate for more support of Ben’s evolving identity.
Community interventions:
- Liaise with Ben’s school counsellor to discuss strategies to minimize and manage discrimination and harassment at school
- Help link Ben with a supportive, caring adult (such as a coach, mentor or youth worker), with whom he can engage, be active, and talk about his challenges
- Connect Ben with community organizations that promote positive connections with adults and prosocial peers, as well as healthy identity development (racial/ethnic and sexual)
Why do health professionals need to know about identity development, acculturation and social integration?
Adaption, acculturation and identity development are complex processes that affect how young newcomers to integrate into life in Canada.
“I feel torn between English and Arabic. Sometimes I miss Arabic so much and I feel like there is a battle in my head … if I want to improve my English skills I would have to stop speaking Arabic and the other way around, and in school or in Canada there is no space for me to develop both”.
Source: “Fresh Voices” report
Ethnic or cultural identity development involves identifying with and relating to a specific group. It is one component of acculturation, which describes changes in a group’s culture or in individual psychology in response to a new environment or other factors. These concepts apply to all immigrants, and are covered in more depth in Adaptation and Acculturation in this resource. Important issues for immigrant adolescents are described below.
Adolescence is a crucial and sensitive period of identity and behavioural development, when patterns of coping, emotional regulation and health-related behaviour become established.5,11 For immigrant adolescents, identity development is complicated by issues of acculturation, racism, discrimination and social marginalization,12,13 as well as the lack of recognition or value placed on pre-immigration life or learning experiences.14
Immigrant adolescents face particular challenges, including: 12,13,15
- Questions of belonging (“Who am I?”, “Where do I fit in ?”)
- Creating positive peer relationships (an important protective factor)
- Conflicting values and belief systems (between or with their culture of origin and Canadian culture)16,17
- Bullying or racism, which can create feelings of alienation13,18
“Most of my friends are from other countries; with them I don’t feel judged.”
“I socialize with the people of my culture because of the stereotypes created, like about terrorism.”
Youth report being told things like, “You should get back to your own country,” or “They should deport you.”
Source: “Fresh Voices” report
The effects of immigration and resettlement experiences. While detailed discussion is beyond the scope of this module, it is worth noting that the conceptualization and use of terms such as “acculturation” and “integration” are controversial.19,20 The role of social determinants of health is increasingly recognized, emphasizing social and structural (rather than individual or cultural) explanations for immigrant health and behaviours.21
Berry defined acculturation as the broader process of psychological changes and adaptations in attitudes, identities and social behaviours in response to intercultural contact and living in a new environment.16 The literature on acculturation and health is complex. Less acculturation can be both protective (the “healthy immigrant effect”) and a risk22,23 for adolescent health-related behaviours.
In Berry’s16,24 multidimensional model of acculturation, there are 4 different acculturation strategies (see Adaptation and Acculturation). Which particular strategy an adolescent adopts may depend on degree of affiliation with (or rejection of) their original and new cultures.13,16 Some evidence suggests that immigrant adolescents with an “integration” profile—affiliating with both their original and their new cultures—have optimal psychological and adaptive functioning.16,24,25 Other studies suggest that those with an inconsistent, confused or incoherent (“diffuse”) acculturation profile and identity development have the most trouble functioning.16
Immigrant adolescents who arrived in Canada before age 10 seem better able to adopt a Canadian identity, rather than continuing to view themselves as foreigners.26 Compared with their first- or second-generation immigrant peers, “1.5-generation” immigrant adolescents (i.e., those who arrive in middle childhood) appear to experience different acculturation and identity challenges.10
Societal attitudes toward immigrants, ethnocultural groups and visible minorities affect identity development. Some youth say that achieving a sense of belonging in Canada is a struggle because of racism and discrimination.13,26 Discrimination experienced by newcomer families has been associated with higher levels of emotional problems in children and younger adolescents.27
Specific questions that any health professional might ask to help assess acculturation, along with other information about next steps, are provided in Immigrant adolescent health Part 2: Guidance for clinicians.
The role of social determinants in immigrant adolescent health
“My parents can’t find appropriate work so both have to work long hours for low pay in jobs that don’t match their skills. It makes it hard to be together as family. My sister is surprised when we eat together.”
“We came to Canada with nothing and we lived in a very small apartment in a rough area in town. My parents had to work minimum wage in order to pay rent and support us.”
Source: “Fresh Voices” report
Adolescent health is strongly affected by broader social determinants such as community and family poverty, income inequality, access to education and employment, and the extent to which families, schools, and peers are safe and supportive.28
Compared to non-immigrant adolescents, immigrant adolescents disproportionately experience social challenges that impact their health. They are more exposed to poverty, substandard housing, food insecurity, social exclusion, unhealthy or unsafe environments, and barriers to accessing health care:29,30
- According to 2006 census data, the low-income rate for families of recent immigrant youth was >3 × than that of Canadian-born youth (46% versus 16%).3
- Immigrant adolescents report experiencing profound stress around the employment challenges their parents encounter in Canada.3
- In 2010, the unemployment rate of immigrant youth (15 to 24 years of age) was higher than that of their Canadian-born peers: 19% versus 14%.31
Risk and protective factors for immigrant adolescent health
A large body of literature demonstrates that early adverse childhood experiences (ACEs), such as abuse, neglect, chronic poverty, family dysfunction, chronic illness, addiction and/or mental illness increase the risks for poor mental health, school problems, delinquency, substance abuse and unhealthy behaviours in youth. Even so, the negative effects of such factors can be moderated significantly by internal and external protective factors.32-34
Other important influences on immigrant adolescent health include pre-migration conditions, the reasons for a family’s migration, migration-related trauma, and details of settlement and integration in Canada. Clinicians should ask about and evaluate such factors in tandem with health risk and protective factors which affect all adolescents. Specific considerations are summarized in Table 1.
| Factor | Evidence |
|---|---|
| Age at migration | Younger age at immigration is associated with a higher risk of mood disorder or anxiety disorber in adults.35 |
| Cultural and personal identity | Exploration of cultural or ethnic identity is a key dimension of acculturation and is intensified among immigrant adolescents. An ethnic or cultural identity crisis may occur when a young newcomer faces uncertainty and difficulties in the process of resolving whether or not to identify strongly – or not at all – with various ethnic identities (also described as marginalization) and is associated with adverse health outcomes.36 |
| Family | While a cohesive and supportive family can be protective, poor family relationships and/or specific living arrangements (such as homestay) can be a risk factor for mental health problems (e.g., suicidal ideation).37-39 (See also Immigrant adolescent health Part 2: Guidance for Clinicians). |
| Pre-migration and migration experiences | Negative pre- or migration experiences – which differ greatly among youth –may be associated with poor mental health.12,13,26 |
| Refugee status | Being a refugee can be a risk factor for poor mental health, such as post-traumatic stress disorder (PTSD).13,26 |
| Discrimination and social exclusion | Marginalization and discrimination are risk factors for maladaptive behaviours and adaptation, while affiliating with both culture of origin and mainstream culture can be protective. For more information, see Adolescent Health Part 2: Guidance for Clinicians. |
| High school completion | The dropout rate for immigrant youth is slightly lower than for Canadian-born youth (6.2% versus 9.1% respectively, in 2009-10). This difference may be due in part to the high value that many immigrant youth and parents place on education, as well as the high concentration of immigrants in large cities, where dropout rates are generally lower than in smaller communities.40 Immigrant adolescents who arrive in Canada before age 9 are significantly more likely to graduate from high school than those who arrive when they are older. Dropout rates among immigrant youth who arrive after age 13 are between 20 and 25%.41 |
| Extracurricular activities | Engaging in meaningful extracurricular activities can be protective for immigrant adolescents, because involvement builds self-esteem.38 |
| Generational status | First-generation immigrant adolescents are at higher risk for emotional symptoms and psychological distress.42,43 Second- and later generation immigrant adolescents are at higher risk for health risk behaviours, including substance use and delinquency, compared to their first-generation immigrant peers.43 |
References
- Chui TWL, Flanders J; Statistics Canada. Immigration and ethnocultural diversity in Canada: National Household Survey, 2016. Ottawa, Ont.: Statistics Canada, 2017.
- Statistics Canada. Census snapshot – Immigration in Canada: A portrait of the foreign-born population, 2006 census. Tech. Rep. 11-008-X. Ottawa, Ont.: Statistics Canada, 2008.
- Shakya Y. Determinants of mental health for newcomer youth: Policy and service implications. Canadian Issues/Thèmes Canadiens 2010:98-102.
- Citizenship and Immigration Canada. Canada facts and figures: Immigration overview. Ottawa, Ont.: Citizenship and Immigration Canada, 2015.
- Sawyer SM, Afifi RA, Bearinger LH, et al. Adolescence: A foundation for future health. Lancet 2012;379(9826):1630-40.
- Ginsburg KR, Carlson EC. Resilience in action: An evidence-informed, theoretically driven approach to building strengths in an office-based setting. Adolesc Med State Art Rev 2011;22(3):458-81.
- Pottie K, Dahal G, Georgiades C, et al. Do first generation immigrant adolescents face higher rates of bullying, violence and suicidal behaviours than do third generation and native born? J Immigr Min Health 2014; Sep 24 [Epub ahead of print DOI: 10.1007/s10903-014-0108-6]
- WHO. Health topics. Adolescent health.
- UNESCO. Learning to live together. What do we mean by “youth”?
- Rumbaut RG. Ages, life stages, and generational cohorts: Decomposing the immigrant first and second generations in the United States. Internat Migr Rev 2004;38(3):1160-205.
- Radzik M. Psychosocial development in normal adolescents. In: Neinstein LS et al, eds. Adolescent Health Care: A Practical Guide, 5th edn. Philadelphia, PA: Lippincott Williams & Wilkins, 2008.
- Ngo H, Schleifer B. Immigrant children and youth in focus. Canadian Issues/Thèmes Canadiens 2005:29-33.
- Salehi R. Intersection of health, immigration, and youth: A systematic literature review. J Immigr Minor Health 2010;12(5):788-97.
- Kilbride KM, Anisef P, Baichman-Anisef E, et al. Between two worlds: The experiences and concerns of immigrant youth in Ontario. Joint Centre of Excellence for Research on Immigration and Settlement – Toronto, 2003.
- Ngo HV. Patchwork, sidelining and marginalization: Services for immigrant youth. J Immigr Refugee Stud 2009;7(1):82-100.
- Berry JW, Phinney JS, Sam DL, Vedder P. Immigrant youth: Acculturation, identity, and adaptation. Appl Psychol 2006;55(3):303-32.
- Güngör D. Immigration and acculturation in adolescence. Encyclopedia on Early Childhood Development. Centre of Excellence for Early Childhood Development, 2011.
- Abada T, Hou F, Ram B. The effects of harassment and victimization on self-rated health and mental health among Canadian adolescents. Soc Sci Med 2008;67(4):557-67.
- Boski P. Five meanings of integration in acculturation research. Int J Intercult Rel 2008;32(2):142-53.
- Li PS. Deconstructing Canada’s discourse of immigrant integration. PCERII Working paper series, no. WP04-03 2003 Prairie Centre of Excellence for Research on Immigration and Integration.
- Acevedo-Garcia D, Sanchez-Vaznaugh EV, Viruell-Fuentes EA, et al. Integrating social epidemiology into immigrant health research: A cross-national framework. Social Sci Med 2012;75(12): 2060-8.
- Flores G, Brotanek J. The healthy immigrant effect: A greater understanding might help us improve the health of all children. Arch Pediatr Adolesc Med 2005;159(3):295-7.
- Santelli JS, Abraido-Lanza AF, Melnikas AJ. Migration, acculturation, and sexual and reproductive health of Latino adolescents. J Adolesc Health 2009;44(1):3-4.
- Berry JW. Acculturation: Living successfully in two cultures. Internat J Intercult Rel 2005;29:697-712.
- Berry JW, Sabatier C. Variations in the assessment of acculturation attitudes: Their relationships with psychological wellbeing. Int J Intercult Rel 2011;35(5):658-69.
- Beiser M, Ogilvie L, Rummens JA, et al. The new Canadian children and youth study: Research to fill a gap in Canada’s children’s agenda. Canadian Issues/Thèmes Canadiens 2005;21-4.
- George MA, Bassani C, Armstrong RW. Influence of perceived racial discrimination on health and behaviour of immigrant children in British Columbia. Int J Pop Res 2012;1-9.
- Viner RM, Ozer EM, Denny S, et al. Adolescence and the social determinants of health. Lancet 2012; 379(9826):1641-52.
- Public Health Agency of Canada. The Chief Public Health Officer’s Report on the state of public health in Canada, 2011, Chapter 3: The health and well-being of Canadian youth and young adults.
- First Call: BC Child and Youth Advocacy Coalition. 2011 Child Poverty Report Card. Vancouver, BC: First Call: BC Child and Youth Advocacy Coalition; 2011.
- Yassad L. The immigrant labour force analysis series: The Canadian immigrant labour market 2008-2011. Ottawa, Ont.: Statistics Canada, 2011.
- Kia-Keating M, Dowdy E, Morgan ML, et al. Protecting and promoting: An integrative conceptual model for healthy development of adolescents. J Adolesc Health 2011;48(3):220-8.
- Boivin M; Royal Society of Canada/CAHS Expert panel reports, 2012. Early Childhood Development.
- Hertzman C. The significance of early childhood adversity. Paediatr Child Health 2013;18(3):127-8.
- Patterson B, Kyu HH, Georgiades K. Age at immigration to Canada and the occurrence of mood, anxiety, and substance use disorders. Can J Psychiatry 2013;58(4):210-7.
- Oppedal B, Roysamb E, Sam DL. The effect of acculturation and social support on change in mental health among young immigrants. Int J Behav Dev 2004;28(6):481-94.
- Cho YB, Haslam N. Suicidal ideation and distress among immigrant adolescents: The role of acculturation, life stress, and social support. J Youth Adolesc 2010;39(4):370-9.
- Smith A, Poon C, Stewart D, et al; McCreary Centre Society. Making the right connections: Promoting positive mental health among B.C. youth. Vancouver, B.C.: McCreary Centre Society, 2011.
- Wong ST, Homma Y, Johnson JL, et al. The unmet health needs of East Asian high school students: Are homestay students at risk? Can J Public Health 2010;101(3):241-5.
- Gilmore J; Statistics Canada, 2010. Trends in dropout rates and the labour market outcomes of young dropouts.
- Corak M; Statistics Canada, 2011. Age at immigration and the education outcomes of children. Analytical studies branch research paper ser. Cat. No. 11F0019M – No. 336.
- Georgiades K, Boyle MH, Kimber MS, et al. Childhood immigration and acculturation in Canada. Bornstein MH, topic ed. In: Encyclopedia on Early Childhood Development. Montreal, Quebec: Centre of Excellence for Early Childhood Development, 2011:1-9.
- Hamilton HA, Noh S, Adlaf EM. Adolescent risk behaviours and psychological distress across immigrant generations. Can J Public Health 2009;100(3):221-5.
Reviewer(s)
Dzung Vo, MD
Kevin Pottie, MD
Reviewer(s)
Last updated: December, 2021