Toxic Lead Exposure: Assessment & Screening
Key points
- Refugee, immigrant and internationally adopted children, especially from resource-poor countries, may have elevated lead levels in their body when they arrive in Canada.
- Sources of lead include environmental soil, air and water contamination as well as consumer products such as cooking utensils, cosmetics and foods.
- Lead exposure may present with acute poisoning, a chronic and variable course or be asymptomatic. Management depends largely on measured blood lead levels.
- A high index of suspicion of lead exposure is needed for newly arrived children. All refugee children and adolescents, including adolescents ≥16 years of age with risk factors for lead exposure, should be screened as soon as possible after arrival. Rescreening in 3-6 months can be considered if the child is ≤6 years of age, risk factors are present or their initial blood lead level was elevated.
Lead in newcomer children
Lead exposure is a concern in young newcomers to Canada, especially in refugee and internationally adopted children. They remain at risk for elevated levels of lead in blood and bone despite declining rates in North American-born children.
As the symptoms of lead toxicity can present in a variety of ways, a high index of suspicion is required for diagnosis. Primary prevention of lead exposure in children is imperative because the harmful effects on neurodevelopment, as well as on cardiovascular, immunological and endocrine function, may be irreversible.1, 2
No known blood lead level (BLL) is considered ‘safe’. In 2012 the U.S. Centers for Disease Control and Prevention lowered their threshold for action from ≥10 μg/dL (≥0.48 μmol/L) to ≥5 μg/dL (0.24 μmol/L).3 The lower threshold is based on evidence indicating that a BLL ≤10 μg/dL has harmful effects on neurodevelopmental, cardiovascular, immunological and endocrine functions. A BLL ≥5 μg/dL “should be investigated thoroughly, and any identified exposure sources should be mitigated as soon as possible.”1
Epidemiology
Patterns, sources and rates of lead exposure vary among and within countries. The burden is greatest in low-income countries; 90% of children with elevated lead levels live in these regions.4 In 2019, the Institute for Health Metrics and Evaluation (IHME) published a map of worldwide lead pollution and children’s BLLs5 (see Figure 1). However, because of limited data, the number of hotspots may be much higher. The number and location of people with elevated lead levels is also changing over time as government policies and economic factors change. It is imperative that care providers attempt to determine the prevalence of lead exposure in a child’s home country to more accurately assess their risk. The IHME also has a more detailed chart outlining estimates of the number of children with BLLs ≥5 µg/dL and ≥10 µg/dL by country. It can be accessed here5 (see Annex). Further information can be found by searching for population-based studies in literature (e.g. Pure Earth) or thorough history-taking where reliable literature is unavailable.
| Figure 1. Map of children’s average BLL (µg/dL) by country.5 |
 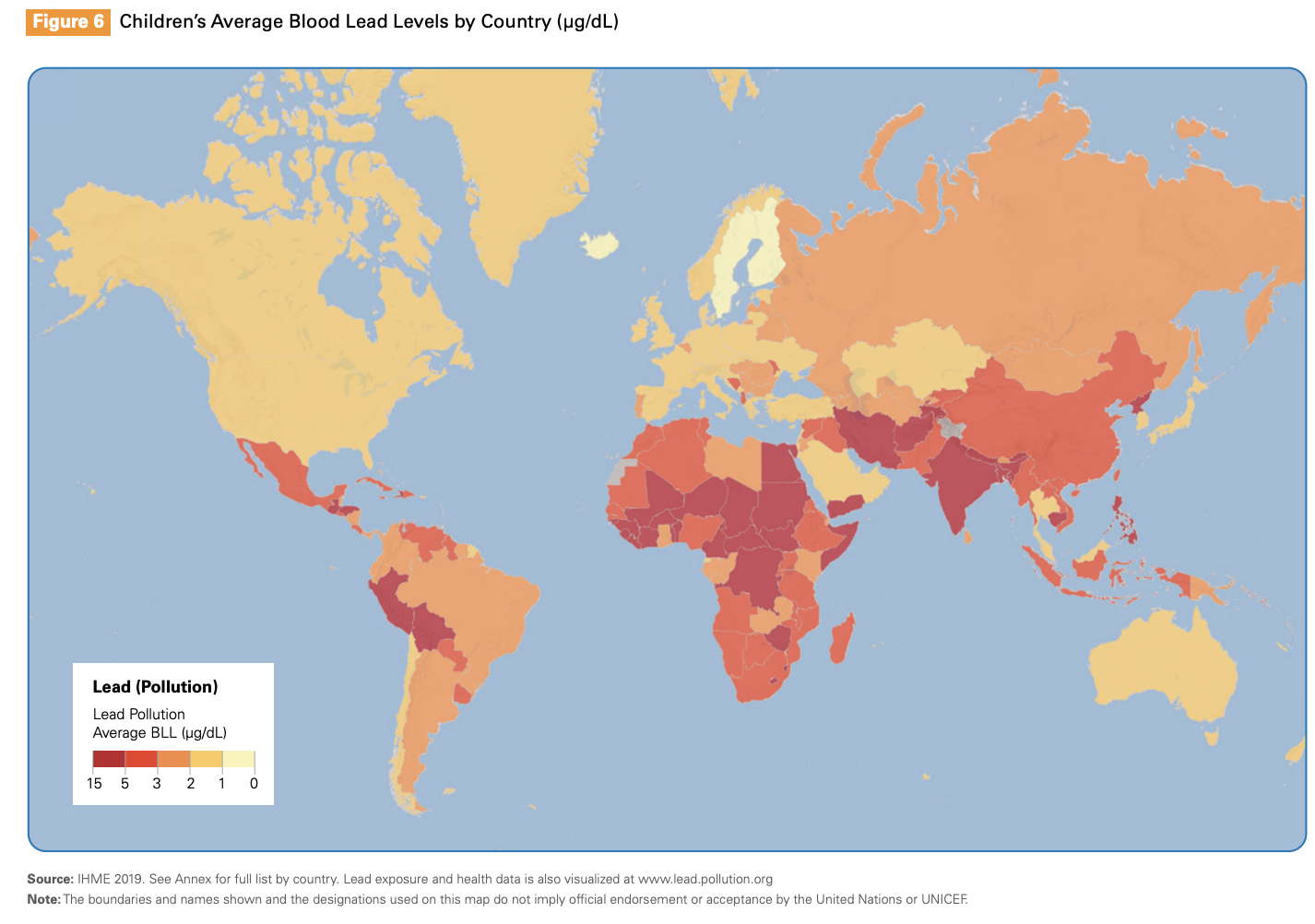 |
While lead levels in North American-born children have been steadily declining in recent years due to greater awareness and policy changes such as the phasing out of leaded gasoline and paint,2,6 refugee children may arrive in Canada with elevated BLLs. Generalizable data on lead exposure in children new to Canada are limited; however, one study from Toronto focused on immigrant and refugee children <6 years of age found that 4.9% of these children had elevated BLLs upon arrival.7 U.S. data indicate that lead exposure rates among refugee children are high.8,9 For example, the prevalence of elevated BLL among refugee children <6 years of age arriving in the U.S. (2002 - 2007) was 8x the national rate.9 Awareness concerning lead exposure risks postarrival increased following the death of a Sudanese child who ingested paint from a 1920’s era home 5 months after reaching the U.S.10 Newcomers often settle in low socioeconomic neighbourhoods, with older homes and sources of environmental lead contamination nearby.8 In Canada, living in older housing can increase exposure to lead as lead plumbing in water lines may have been used until 1950 and lead-based paint until 1976.11
Sources of lead exposure
Sources of lead vary depending on the region of the world but may include leaded gasoline, used batteries, leaded paint, cookware and cosmetics.11-19 Refugees are at increased risk when refugee camps are located on or close to contaminated sites.20 Useful information on sources of lead is provided online by Health Canada.11
Lead exposures can occur before and after migration:2,11-19
- Environmental exposures pre-migration: Children, especially from low-income countries, may be at risk of environmental exposure pre-migration from various sources. Leaded paint chips and fumes from vehicles using leaded gasoline can contaminate the soil that children play on and the air they breathe. Emissions from industries such as battery and electronic waste recycling, smelting and mining also contribute to this pollution. In a similar way, drinking water can become contaminated. Depending on where children immigrate from, they may have also been involved with informal “work” such as metal scavenging or electronic waste recycling. Also, consumer products such as batteries, cosmetics and cooking utensils may contain lead that can be inhaled, ingested or absorbed through dermal contact.
- Environmental exposures post-migration: Newcomer families may settle near industrial areas or live in older housing, posing a risk of exposure through leaded paint, industrial emissions and lead-contaminated water from old water service lines. Additionally, some families continue to use lead-contaminated products from their country of origin (e.g. traditional therapies and imported food or cosmetics).
A malnourished child may be at increased risk of lead absorption. Refugee children in particular are often malnourished and may continue to be malnourished once in Canada. If their diet is low in lead-protective nutrients such as iron and calcium over a long period, increased intestinal lead absorption is a concern.
Common sources of lead exposure in children include:2,11-19,21-22
Food and cosmetics:
- Ceramic or metal utensils, dishes and pots
- Drinking water (from pipes and storage containers where lead was used as a solder material)
- Ingredients or packaging of certain food (e.g. game meat killed with leaded ammunition), spice (e.g. adulterated turmeric) and candy products
- Cosmetics (such as kohl (al-khal, kajal) and surma)
- Traditional medicines (notably from the Middle East, Southeast Asia, India, the Dominican Republic or Mexico)
Environments and industry:
- Emissions, especially from mining or smelting sites, that contaminate bodies of water, soil and air
- ‘Cottage’-based industries (e.g. breaking up batteries or metal ore)
- Leaded gasoline exhaust in high-traffic areas or in soil contaminated by leaded gasoline
- Emissions from burning fossil fuels or waste
A useful list of sources of lead is provided online by Health Canada.11
Clinical presentation
Children experiencing chronic, low-level lead exposure are often asymptomatic 1,23,24 and may therefore go undiagnosed. Signs and symptoms of lead exposure, when they do occur, can also be quite vague and non-specific (see Table 1).1,24 Acute symptoms may occur, particularly when the BLL is ≥10 μg/dL.25 At BLLs ≥60 μg/dL, children may experience headaches, abdominal pain, anorexia, constipation, clumsiness, agitation and lethargy.26 Symptomatic lead exposure should be treated as a medical emergency.27
| Gastrointestinal issues |
Abdominal pain Constipation Nausea Vomiting |
| Impaired neurological development |
Behavioural changes such as inattention and hyperactivity Cognitive delay Hearing impairment Speech Delay Poor balance Seizures Coma |
| Impaired growth and development |
Decreased height Delayed sexual maturation |
| Other | Increased dental caries |
Risk factors and screening
Currently, there are no Canadian screening guidelines for lead exposure in young newcomers, but most experts believe that all refugee and internationally adopted children and youth should be screened as soon as possible postarrival.25 If the child is ≤6 years of age, the initial BLL was elevated, or risk factors of lead exposure are suspected or present, screening should be repeated in 3-6 months.25 Additionally, all pregnant or lactating females should be screened.
Screening should be performed for children with risk factors for lead exposure. Such risk factors include:1,34
- Residence in a house or apartment building built before 1960 within the past 6 months , especially when water is supplied by lead piping or original paint is present, peeling or chipped, or the dwelling is under renovation;
- A sibling, housemate of playmate with a history of lead poisoning;
- A tendency to mouth or eat paint chips or painted objects;
- Emigration from a country with a higher prevalence of elevated BLLs than Canada; and
- Any combination of the above factors with the presence of a known or suspected neurodevelopmental disorder.
Management
There are no specific Canadian guidelines for managing children with an elevated BLL, however, the Canadian Pediatric Society recently published a practice point for use by care providers, which can be found here.
Recommendations for care are based largely on BLL levels .1 Any time the measured BLL is ≥5 μg/dL, the Pediatric Environmental Health History35 should be activated to obtain further information and attempt lead source identification.
It is important to remember that the measured BLL only reflects recent exposures, therefore a BLL ≤5 μg/dL should not rule out lead exposure.1 Investigations should also generally include a CBC, as well as ferritin, calcium, albumin and protein levels.1 A nutritional assessment and optimization is important as well. Iron and calcium are lead-protective and are more readily absorbed if taken with Vitamin C, so fresh fruit at every meal is indicated.1 Management of any BLL ≥5 μg/dL warrants a full neurodevelopmental assessment and follow-up. Remeasurement of any elevated BLL is warranted, and timing varies based on the initial BLL detected.1 Chelation therapy is generally not considered unless the BLL is ≥44 μg/dL.1
Prevention
Clinicians can help to prevent lead exposure in young newcomers to Canada by educating parents about potential harms and common sources of exposure.27 Patients should be directed to reliable sources of information. Because sources may be culture-specific (e.g. traditional remedies, therapies or foods), it is important to explore possible risks in a culturally sensitive manner36 and address potential barriers to adopting medical advice, such as living in a substandard environment. Additionally, prenatal lead exposure should be prevented by counselling women prior to or during pregnancy on avoiding lead exposure.34 Finally, physicians and other leaders in healthcare should advocate for legislative change where possible to assist in primary prevention efforts.
Selected Resources
Clinicians can direct parents to these online resources:
- Health Canada. Lead and Human Health
- Health Canada. Reduce your exposure to lead.
- CDC. Lead Poisoning Prevention in Newly Arrived Refugee Children: Tool Kit
- CDC. Fact sheets on lead poisoning prevention information (English and Spanish) and Prevention tips.
References
- Buka I, Hervouet-Zeiber, C. Lead toxicity with a new focus: Addressing low-level lead exposure in Canadian children. Pediatrics and Child Health 2019;24(4):293.
- CDC, Advisory Committee on Childhood Lead Poisoning Prevention. Low level lead exposure harms children: A renewed call for primary prevention. Atlanta, GA: CDC; January 4, 2012.
- CDC. Blood Lead Reference Value. Atlanta, GA: CDC, December 2020.
- WHO. Childhood lead poisoning. Geneva, Switzerland: WHO, 2010.
- UNICEF and Pure Earth. The Toxic Truth: Children’s Exposure to Lead Pollution Undermines a Generation of Future Potential. New York, United States: UNICEF and Pure Earth. July 2020.
- Statistics Canada. Health fact sheet: Blood lead concentrations in Canadians, 2009 to 2011. Catalogue no. 82‑625‑X. April, 2013.
- Salehi L, Lofters AK, Hoffmann SM, et al. Health and growth status of immigrant and refugee children in Toronto, Ontario: A retrospective chart review. Pediatrics and Child Health 2015;20(8):e38-e42.
- Geltman PL, Brown MJ, Cochran J. Lead poisoning among refugee children resettled in Massachusetts, 1995 to 1999. Pediatrics 2001;108(1):158-62.
- Proue M, Jones-Webb R, Oberg C. Blood lead screening among newly arrived refugees in Minnesota. Minn Med 2010;93(6):42-6.
- CDC. Fatal pediatric lead poisoning–New Hampshire, 2000. MMWR Morb Mortal Wkly Rep 2001;50(22):457-9.
- Health Canada. Lead Information Package - Some Commonly Asked Questions About Lead and Human Health. April 2009.
- Clune AL, Falk H, Riederer AM. Mapping global environmental lead poisoning in children. J Health Pollution 2011;1(2):14-23.
- Kaul B, Sandhu RS, Depratt C, et al. Follow-up screening of lead-poisoned children near an auto battery recycling plant, Haina, Dominican Republic. Environ Health Perspect 1999;107(11):917-20.
- Ling S, Chow C, Chan A, et al. Lead poisoning in new immigrant children from the mainland of China. Chin Med J (Engl) 2002;115(1):17-20.
- López-Carrillo L, Torres-Sánchez L, Garrido F, et al. Prevalence and determinants of lead intoxication in Mexican children of low socioeconomic status. Environ Health Perspect 1996;104(11):1208-11.
- Rahbar MH, White F, Agboatwalla M, et al. Factors associated with elevated blood lead concentrations in children in Karachi, Pakistan. Bull World Health Organ 2002;80(10):769-75.
- Schwartz J, Levin R. The risk of lead toxicity in homes with lead paint hazard. Environ Res 1991;54(1):1-7.
- Stroh E, Lundh T, Oudin A, et al. Geographical patterns in blood lead in relation to industrial emissions and traffic in Swedish children, 1978-2007. BMC Public Health 2009;9:225.
- Suplido ML, Ong CN. Lead exposure among small-scale battery recyclers, automobile radiator mechanics, and their children in Manila, the Philippines. Environ Res 2000;82(3):231-8.
- Brown MJ, McWeeney G, Kim R, et al. Lead poisoning among internally displaced Roma, Ashkali and Egyptian children in the United Nations-Administered Province of Kosovo. Eur J Public Health 2010;20(3):288-92.
- CDC. Childhood Lead Poisoning Prevention: International Adoption. Atlanta, GA: CDC, August 2019.
- Forsyth JE, Nurunnahar S, Islam SS, et al. Turmeric means “yellow” in Bengali: Lead chromate pigments added to turmeric threaten public health across Bangladesh. Environmental Research 2019;179(A):108722.
- CDC. Medically oriented fact sheet. Lead poisoning prevention and treatment recommendations for refugee children. Refugee tool kit. Atlanta, GA: CDC, 2009.
- Warniment C, Tsang K, Galazka SS. Lead poisoning in children. Am Fam Physician 2010;81(6):751-7.
- CDC. Lead screening during the domestic medical examination for newly arrived refugees. Atlanta, GA: CDC, January 7, 2020.
- Canfield RL, Henderson CR Jr, Cory-Slechta DA, et al. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N Engl J Med 2003;348(16):1517-26.
- American Academy of Pediatrics (AAP) Committee on Environmental Health. Lead Exposure in Children: Prevention, Detection, and Management. Pediatrics 2005;116(4):1036-46.
- Gemmel A, Tavares M, Alperin S, et al. Blood lead level and dental caries in school-age children. Environ Health Perspect 2002;110(10):A625-30.
- Needleman HL, Riess JA, Tobin MJ, et al. Bone lead levels and delinquent behavior. JAMA 1996;275(5):363-9.
- Shukla R, Dietrich KN, Bornschein RL, et al. Lead exposure and growth in the early preschool child: A follow-up report from the Cincinnati Lead Study. Pediatrics 1991;88(5):886-92.
- Sood A, Midha V, Sood N. Pain in abdomen—do not forget lead poisoning. Indian J Gastroenterol 2002;21(6):225-6.
- Williams PL, Sergeyev O, Lee MM, et al. Blood lead levels and delayed onset of puberty in a longitudinal study of Russian boys. Pediatrics 2010;125(5):e1088-96.
- Wu T, Buck GM, Mendola P. Blood lead levels and sexual maturation in U.S. girls: The Third National Health and Nutrition Examination Survey, 1988-1994. Environ Health Perspect 2003;111(5):737-41.
- Abelsohn AR, Sanborn M. Lead and children: Clinical management for family physicians. Can Fam Physician 2010;56(6):531-5.
- WHO. Children’s Environmental Record - “GREEN PAGE”. Geneva, Switzerland, WHO.
- Vo D, Mayhew M. Cultural Competence for Child and Youth Health Professionals. Canadian Pediatric Society: Caring for Kids New to Canada. April 2018.
Reviewer(s)
Anne Hicks, MD
Contributor(s)
Irena Buka, MD
Mikayla Gray, MD
Catherine Hervouet-Zieber, MD
Last updated: March, 2021